
Summary
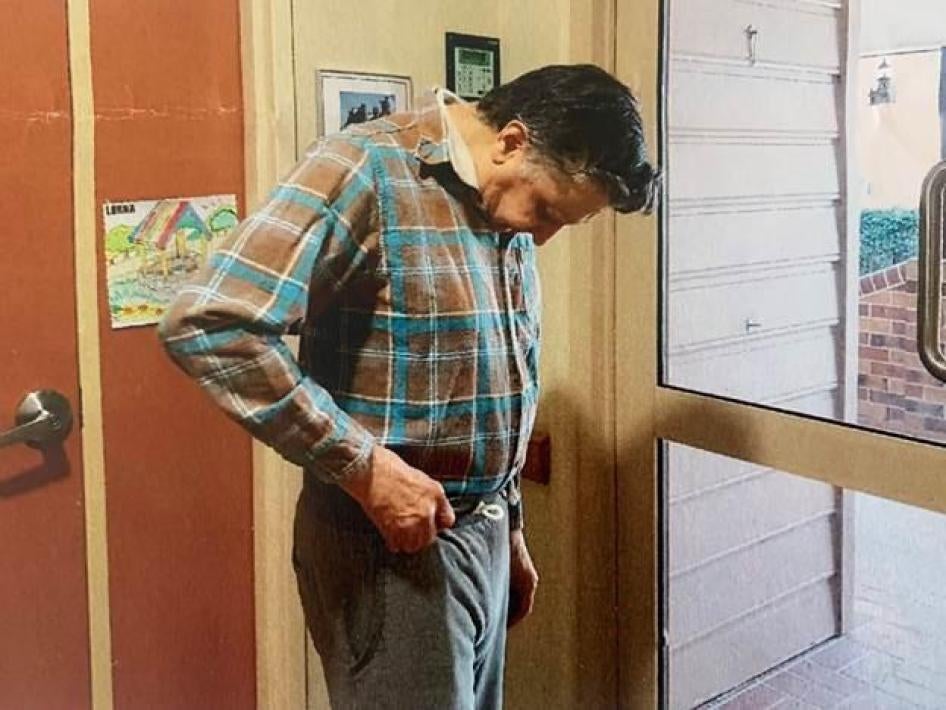
At that stage he couldn’t walk, only shuffle, he was very, very depressed, just crying all the time. And he couldn’t swallow… He would say, “My mind is a hell to me.” He wouldn’t be engaged in a conversation… All his symptoms are side effects of the antipsychotics, and they disappeared after he went off [them]. – Susan Ryan describing her father in 2013, June 2019
Susan Ryan was describing Ray, her 78-year-old father, when he was being chemically restrained in an aged care facility in 2013. Ray is one of approximately 450,000 people estimated to be living with some form of dementia in Australia. Dementia is a progressive, degenerative brain disease – associated with loss of memory and other cognitive abilities – that tends to occur in older age. Over half of the people living in aged care facilities have dementia. In Australia, staff at aged care facilities are giving older people with dementia drugs to control their behavior even though the drugs are not required to treat medical symptoms – a practice known as chemical restraint.
Restraining older people with drugs can have grave consequences. One woman described her grandmother, who in 2018 was living in an aged care facility in southern Queensland:
“Everything about her, her health, her spirit, declined after that drug. We went to see her after the meds, and she couldn’t hold a conversation, she was dropping off to sleep, [just] like that. She wouldn’t get up to go to the toilet until the last second because she was so tired.”
These and other relatives of older people living with dementia in aged care facilities described a dramatic deterioration in the conditions of their family members, including formerly energetic, talkative people who became lethargic and, in some cases, unable to speak. Many said that their relatives slept heavily, often for long periods, and could not be awakened without difficulty. They experienced serious weight loss, often because they were not able to stay awake long enough to eat.

Medications should only be given when they have a therapeutic value. Medication for the purposes of controlling behavior without a therapeutic purpose is chemical restraint. The long-term, continual use of this practice on older people with dementia in aged care facilities in Australia appears to be driven by a number of factors, including understaffing of aged care facilities and inadequate training in dementia support, leading to an inability to appropriately support the needs of people with dementia. For understaffed facilities, chemical restraint can make managing people with dementia easier, especially when staff lack adequate training in supporting people with dementia. “They don’t have enough staff or supervision so they knock them out,” the daughter of a woman with dementia told Human Rights Watch. In many facilities, inadequate staff and training make it almost impossible to take an individualized, comprehensive approach to supporting people with dementia. Many aged care facilities have staffing levels well below what experts consider the minimum needed to provide appropriate care.

This report is based on interviews with family members, doctors, nurses, and advocates, and documents the use of medications as chemical restraint in 35 aged care facilities in three states in Australia: Queensland, Victoria, and New South Wales. In all three states, Human Rights Watch research indicated that older people were restrained with sedatives and antipsychotic medications. The report is based on interviews with 89 individuals, including 37 family members of older persons who are living in aged care facilities or deceased (plus one older person living in an aged care facility), aged care facility staff, doctors, nurses, aged care experts and disability rights experts, advocacy organizations, and government officials between April 2018 and August 2019.
Human Rights Watch documented the use of various drugs used in chemical restraint, including antipsychotic drugs, benzodiazepines, and sedative-hypnotic drugs, sometimes known as “tranquilizers,” “sleeping pills,” or “sedatives”; and opioid analgesics, also known as narcotic painkillers.
Clinical studies in the United States have found that antipsychotic drugs increase the risk of death in older people with dementia. Benzodiazepine use in older people is associated with increased risks of falls, pneumonia, and death. The government of Australia has not approved the use of many of these drugs in older people, citing these studies.
As best as Human Rights Watch can determine, staff in the aged care facilities where we conducted research did not seek or secure informed consent prior to giving these medications. Informed consent requires a decision based on a discussion of the purpose, risks, benefits, and alternatives to a medical intervention, as well as the absence of pressure or coercion in making the decision. Individuals receiving medication should only receive it after they have given their free and informed consent in accordance with international human rights standards.
In addition, family members who have powers of attorney (legal authority to act on another’s behalf) to make decisions on behalf of their relatives in aged care facilities told Human Rights Watch that facility staff did not seek their informed consent for the medications used as chemical restraints. Many relatives said they only learned that their relatives had been given medications after they received pharmacy bills listing the medications. For example, one woman described her shock and confusion after receiving a pharmacy bill listing an antipsychotic medication, among others, that staff were giving to her husband in an aged care facility in northern Queensland. She told Human Rights Watch that the facility had not discussed this with her, much less sought her informed consent, even though she holds power of attorney for her husband.
When families confronted facilities with requests for the removal of chemical restraints, they said they were met with intimidation and retaliation.
Chemical restraint is not a necessary or last-resort option. Clinical studies have shown that non-medical interventions focused on an individual’s unique qualities as a person and building and nurturing relationships are effective tools for addressing symptoms of dementia, including agitation and aggression. These symptoms can be distressing for the people who experience them, their families, and aged care facility staff.
Positive interventions include exercise, music, and redirection to a different activity. Human Rights Watch documented several cases in which family members described how relatives with dementia who were taken off medications used to restrain them regained much of their vitality, once again talking and interacting, and staying awake during the day. However, some relatives continued to experience the negative physical and cognitive impacts consistent with the effects of chemical restraints, such as the loss of muscle strength and the inability to swallow.
Australia’s existing legal and regulatory framework is inadequate to protect older people in aged care facilities from chemical restraint; it explicitly allows it. Until the introduction of a new regulation by the Commonwealth Minister for Senior Australians and Aged Care that came into effect on July 1, 2019, there was no regulation of chemical restraint in aged care at all. The regulation purports to minimize the use of physical and chemical restraint, but it does not because it does not prohibit chemical restraint, guarantee the right to informed consent, or provide for a complaint mechanism when a person has been chemically restrained.
Under international human rights law, governments are obligated to respect the inherent dignity of persons with disabilities, including older people, by acknowledging them as persons on an equal basis with others. This includes recognizing that they have the right to live independently in the community without being forced to live in an institution, and to have all their human rights protected if they choose to be in institutions such as aged care facilities. Governments should also prevent discrimination and abuse against people with disabilities and remove barriers that prevent their full inclusion in society.
Australia’s Aged Care Quality and Safety Commission, the agency that regulates aged care and handles complaints about aged care, closed 5,738 complaints in the fiscal year ending June 30, 2018. Seventy-five percent of the complaints were about residential aged care; the remainder came from other areas it oversees, such as home care. Those whom Human Rights Watch interviewed who had attempted to use the system in 2016, 2017, and 2018 did not find it to be an effective mechanism to challenge facilities’ use of chemical restraints on their family members.
The provision of any medication without informed consent violates the right to informed consent to medical treatment and interventions and the right to the highest attainable standard of health. It violates human dignity, bodily integrity, and equality. The use of drugs as a chemical restraint could constitute cruel, inhuman, and degrading treatment under international law.
Appropriate support for people living with dementia will require legislative and regulatory change and enforcement by prohibiting chemical restraint as well as increasing numbers of trained staff, particularly as the older population of Australia continues to increase. Inaction is not an option. The consequences of inadequate legal and regulatory frameworks to prevent chemical restraint are needless suffering, increased disability, and even death.
The Australian government should end the use of chemical restraints as a means of controlling the behavior of older people in aged care. The government should develop support and interventions, including person-centered care, for persons experiencing agitation, emotional distress, or challenging behaviors in aged care facilities. Any new law should also ensure informed consent for all treatment and ensure independent monitoring and effective, accessible, independent complaint mechanisms, including for individuals in aged care facilities and their families.
Key Recommendation
Parliament should enact legislation to prohibit the use of chemical restraints as means of controlling the behavior of older people with dementia or for the convenience of facility staff. The legislation should include:
- Mandatory training for all aged care facility staff in dementia and alternative methods and skills to de-escalate unwanted behavior and support the needs of people with dementia;
- Adequate minimum staffing levels to provide support to older people; and
- Adequate enforcement mechanisms to protect older people’s rights.
Methodology
This report is based on Human Rights Watch interviews with 89 people conducted between April 2018 and August 2019 in the Australian Capital Territory; in and around the cities of Brisbane and Cairns in Queensland; in and around Melbourne, Victoria; and in and around Sydney in New South Wales. The three states were selected based on their high populations of older people and number of aged care facilities. Human Rights Watch conducted additional phone interviews from January 2019 through August 2019.
This report focuses on the human cost of Australian aged care facilities’ use of non-medically required drugs to control the behavior of older people with dementia. Many older people in aged care facilities are at risk of this abuse.
Our research documented the accounts of family members who observed older people with dementia under chemical restraint in aged care facilities. We interviewed them about what changes they saw, what they learned about their family member’s drug intake, and whether they raised any concerns with facility staff or the government complaints agency. Some of the people interviewed requested anonymity. All instances where pseudonyms have been used are referenced in the footnotes. In some cases we have withheld additional identifying information to protect a person’s identity.
We found interviewees through Australian state aged care advocacy organizations, dementia advocacy organizations and advocates, and referrals from people we interviewed. In most cases, relatives of people in aged care had contacted organizations for advice, legal representation, or other support. Those organizations then facilitated introductions.
For this reason, the families of older people interviewed for this report cannot be said to reflect the most isolated and at-risk people in aged care facilities: people who are on their own, without family or friends visiting or communicating with the facility staff, and who have disabilities that impair their ability to communicate or advocate on their own behalf.
We interviewed 37 relatives of older people aged 59 to 103 years. We interviewed one older person who has dementia and experienced chemical restraint. We did not conduct interviews with other older people who had experienced chemical restraint. Some people had passed away by the time of our interview with a family member, some had been taken off chemical restraints, and some were still being restrained.
We interviewed people in the locations they indicated as most comfortable to them: in their homes, at advocacy organization offices, and in cafes or other public locations. We conducted three interviews in aged care facilities with relatives of a person with dementia, with the person who has dementia present. We conducted one interview with a person with dementia in an aged care facility. We conducted interviews in private so that individuals could speak without fear of potential retaliation from aged care facility staff or relatives.
Human Rights Watch obtained the informed consent of each interviewee; explained the aim of the research; how information collected would be used; and informed them that they could discontinue the interview at any time and could decline to answer questions without consequence. Human Rights Watch provided no personal service or benefit and told interviewees that their participation was voluntary, and their identities would be kept confidential where requested.
We interviewed 36 experts, including three doctors, two facility managers, one director of nursing, four professional advocates, two nurses, one physiotherapist, and one pharmacist. We also interviewed lawyers, academic researchers, professors, and representatives from advocacy and interest groups.
In order to obtain the perspectives of aged care facilities, Human Rights Watch sent letters requesting to meet with facility managers at 21 facilities chosen at random in Queensland, New South Wales, and Victoria. We received two responses: one declined, the other accepted. We interviewed one other facility administrator, as well as other staff members speaking in their personal capacity, not for their institution. We did not seek interviews with facilities where family members told us their relatives were facing chemical restraint to avoid any risk of reprisals.
Human Rights Watch shared some of the key findings of this report with Leading Age Services Australia, a trade association for aged care providers; Aged and Community Services Australia, a trade association for non-profit aged care providers; and the Aged Care Guild, requesting their perspectives. Leading Age Services Australia and Aged and Community Services Australia responded, and we met with Aged and Community Services Australia.
We also met with 15 government officials including from the Department of Health, Office of the Public Advocate for Victoria, the Australian Human Rights Commission, the Queensland Public Guardian, and the Department of the Prime Minister and Cabinet. We met with advisors to the Minister for Aged Care and the Attorney General. We wrote a letter requesting a response from the Department of Health. The department’s response is reflected in relevant sections of this report and is also included in Annex I. We requested a meeting and wrote a letter requesting a response from the Aged Care Quality and Safety Commission, the primary agency responsible for monitoring aged care in Australia, in respect of this report’s findings, but had not heard back at time of writing.
Responses received are reflected in the report. Our letters and correspondence are included in the annex.
I. Background
Overview of Aged Care in Australia
Australians aged 65 and over make up about 15 percent of the total population of Australia. By 2057, it is projected they will make up 22 percent of the population.[1]
Australia’s Aged Care Act 1997 defines residential aged care as: personal care or nursing care, or both personal care and nursing care, that is provided to a person in a residential facility in which the person resides, including appropriate staffing to meet the nursing and personal care needs of the person; meals and cleaning services; and furnishings, furniture and equipment for the provision of that care and accommodation.[2]
Care is generally provided by personal carers, enrolled nurses, and registered nurses.[3] There is no federal legislative requirement for aged care facilities to have on-site nurses 24 hours per day.[4] The number and type of staffing is not regulated in aged care facilities in Australia.[5] Such ratios of support are regulated for other settings, such as childcare settings and hospitals.[6] There is no national minimum standardized training requirement for aged care personal carers, including on dementia care.[7]
As of June 30, 2018, there were 2,695 residential aged care facilities in Australia, with capacity for 207,100 people.[8] More than half of the people living in aged care facilities in Australia have dementia.[9] New South Wales has 882 aged care facilities, Victoria has 760, and Queensland, 456.[10] About 45 percent of these facilities are for-profit, 40 percent are religious and charitable organizations, 13 percent are community-based organizations, and about three percent are run by state, territorial, and local governments.[11]
Aged care in facilities is paid for by both the Australian government and by contributions from the residents. The government pays “subsidies and supplements” to approved providers for each resident receiving care under the Aged Care Act, based on an assessment of residents’ support needs.[12] Most residents will pay at least a basic fee every two weeks of AU$576 (US$393), plus, in some cases, additional contributions based on income and assets.[13] For the fiscal year 2017-18, government contributions averaged AU$65,600 (US$44,784) per permanent facility resident (as opposed to short-term residents).[14]
The total government expenditure on aged care in fiscal year 2017-2018 was AU$18.6 billion (US$12.7 billion), according to the Aged Care Financing Authority, an independent agency providing independent advice to the Australian government on the sustainability of the aged care sector.[15] Of this, 66 percent went to residential care; 12 percent to home care; 17 percent to home support; and 2.7 percent to flexible aged care, such as therapy after hospital stays, rural health, and aged care support and short-term programs.[16]
Older People “Prefer to Live at Home”
In 2015, the Australian government’s Productivity Commission, which provides research and advice on issues affecting the welfare of Australians, published a research paper analyzing housing decisions of older people.[17] The data revealed that older people prefer to “age in place,” meaning remain at home in their local community.[18] Most older Australians live in private residences (their own homes), and about 80 percent own their homes.[19] The research also revealed that “the majority of older people are satisfied with their dwellings.”[20]
The Commission recommends that the government provide greater support for people to remain in their homes and receive necessary support and care there because older people have expressed this preference. The Commission also notes that this policy may align with the government’s fiscal sustainability objectives to rein in spending, according to the report: “Although the care needs are typically higher for residential aged care, ultimately delivering home care requires much less public funding.”[21] The government has announced increased funding for services to enable older people to continue to live independently in their own homes.[22]
Dementia
Globally, in 2017, nearly 50 million people were estimated to be living with dementia.[23] Alzheimer’s disease is the most common cause of dementia contributing to an estimated 60 to 70 percent of all dementia.[24] In Australia, 447,115 people are estimated to be living with some form of dementia.[25]
Dementia is “the loss of cognitive functioning—thinking, remembering, and reasoning—
and behavioral abilities to such an extent that it interferes with a person's daily life and activities.”[26] It may change functioning of memory, language, attention, emotion and self-management, among other things. [27]
Dementia-related symptoms may result from changes in the body’s nervous system associated with dementia or from an external or underlying situation such as pain or personal needs.[28] Dementia is often accompanied by irritability, agitation, aggression, hallucinations, delusions, wandering, disinhibition, anxiety, and depression.[29] These symptoms may be a response to unmet physical needs like being hungry, thirsty, or cold, or to “environmental triggers,” such as being ignored. Alternatively, symptoms may be “consequences of a mismatch between the environment and patients’ abilities to process and act upon cues, expectations and demands.”[30] They can be distressing for the people who experience them, their families, and aged care facility staff.
Person-Centered Care
Research has found that person-centered care, focused on an individual’s unique qualities as a person and building and nurturing relationships between the individual and others, is an effective non-pharmacological intervention for improving symptoms of dementia, including agitation and aggression.[31] Non-pharmacological interventions can include physical exercise, music therapy, massage, redirection, and others. Several studies have confirmed the positive results of music therapy.[32] Other non-pharmacological interventions includes reducing boredom, pain, loneliness, and similar experiences by changing a person’s activities, surroundings, opportunities, and access to relationships; creating individualized sleep, hygiene, bathroom, and other daily routines that the person prefers; or ensuring staff are consistent and familiar with the individual.[33]
Studies from the United States have found that people with dementia treated with person-centered care interventions demonstrated signs of improved quality of life, decreased agitation and other “challenging behaviors,” improved sleep patterns, and maintenance of self-esteem.[34]
The World Health Organization (WHO) has found that aggressiveness and unwanted behavior can often arise when individuals are constrained by the inherently rigid nature of a facility that does not give adequate attention to an individual’s will and requirements.[35] The WHO is designing programs to train facility staff to prevent situations that can escalate into aggressiveness, violence, and behavior that could result in self-harm. One key element is creating an institutional environment that recognizes individual needs and requirements and provides services in a timely and dignified manner. Other alternatives are designing individualized plans to understand and recognize triggers, early warnings, and tense situations.[36] The Australian government does not currently require these practices.
Chemical Restraint
Chemical restraint is defined in Australia’s 2019 regulation on minimizing restraints as “a restraint that is, or that involves, the use of medication or a chemical substance for the purpose of influencing a person’s behaviour, other than medication prescribed for the treatment of, or to enable treatment of, a diagnosed mental disorder [mental health condition], a physical illness or a physical condition.”[37] The WHO defines it similarly: “medication which is not part of the person’s treatment regimen and is used to restrict the freedom of a person’s movement and/or control their behaviour.”[38] Some countries such as the United States have prohibited chemical restraint in aged care facilities.[39]
Recognition of the Problem of Chemical Restraint in Aged Care
Over the years, policy and legal experts in Australia have criticized the use of chemical restraint in aged care facilities. High-profile cases have helped spark public awareness about the dangers of over-medicating people with dementia. Bob Spriggs, 66, died in February 2016 from an overdose of an atypical antipsychotic drug at an aged care facility in Oakden, South Australia. He had dementia and Parkinson’s disease. [40] In 2017, a government regulatory review found that, “While the situation at Oakden is far from typical, the circumstances that led to it are certainly not unique.”[41] In September 2018, a widely watched television news program, 4 Corners, investigated a range of serious abuses in aged care facilities across Australia, including chemical restraint.[42]
Medical and legal experts have also raised the issue of chemical restraint and the lack of effective regulation. The Australian Society for Geriatric Medicine noted in 2005:
The problem of … drug use is a very serious and significant one in residential care facilities… The answer to behavioural problems in patients with dementia, for example, is not to give them antipsychotic medications but to put in place [sic] appropriate behavioural and environmental strategies.[43]
In February 2019, the acting state coroner in Victoria published his findings in relation to the death of Margaret Barton in an aged care facility at the age of 83. The coroner found “there is sufficient correlation between Mrs. Barton’s multiple falls and the Oxazepam, to conclude that the medication regime contributed to her physical decline and death.”[44]
And the Australian Law Reform Commission noted in its 2017 report on elder abuse that “the use of restrictive practices…can deprive people of their liberty and dignity—basic legal and human rights.”[45] The Australian government’s Review of National Aged Care Quality Regulatory Processes in 2017, noted that in aged care facilities, “There are pressures on all sides that promote antipsychotics as a ‘quick fix,’ and once commenced, a ‘set and forget’ mentality can result.”[46] It also found that, “The standards [for aged care facility accreditation] do not [regulate] adequately in the area of restrictive practices.”[47] In 2017, the Queensland Office of the Public Advocate concluded that: “[T]he Aged Care Act does not currently act as an effective mechanism for reducing or regulating restrictive practices in the aged care sector.”[48]
Medicines as Chemical Restraints
Different drugs can be used as chemical restraints. These include antipsychotics, sometimes known as neuroleptics, used to treat symptoms of delusions and hallucinations; or, benzodiazepines and sedative-hypnotic drugs, sometimes known as “tranquilizers,” “sleeping pills,” or “sedatives”; and others, like opioid analgesics, known as narcotic painkillers. Benzodiazepine use in older people is associated with increased risks of falls, pneumonia, and death.[49] Australia’s government subsidizes the cost of these medications.[50]
Scientific studies have also documented the use of these drugs in aged care facilities in the country. A May 2018 study of 12,157 residents in 150 aged care facilities in Australia found that 22 percent were taking antipsychotics every day.[51] A 2010 study of aged care residents in 40 aged care homes throughout Tasmania found that 21 percent of residents were taking antipsychotics, and 43 percent were taking anti-anxiety or hypnotic medicines (commonly referred to as “sleeping pills”).[52] Other studies have estimated even higher rates of use in some parts of Australia, including a finding of 57,130 prescriptions of antipsychotics prescribed for every 100,000 people over 65 years of age in Yarra, Victoria in 2013-14.[53]
Antipsychotic Medications
Antipsychotics increase the risk of death in older people with dementia, according to at least 17 placebo-controlled clinical studies of the drugs, mostly conducted in the US.[54] The causes of death varied, but most were related to heart failure or infections like pneumonia.[55]
Aside from raising the risk of death, the side effects of antipsychotics can include severe nervous system problems, neuroleptic malignant syndrome (a life-threatening reaction associated with severe muscular rigidity, fever, and altered mental status); tardive dyskinesia (characterized by stiff, jerking movements that may be permanent once they start and whose likelihood of onset increases the longer antipsychotic drugs are taken); high blood sugar and diabetes; and low blood pressure, which causes dizziness and fainting.[56] Other side effects can include increased mortality, cerebrovascular events (stroke), cardiovascular effects, blood clots, central and autonomic nervous system problems, visual disturbances, metabolic effects, fall risk and hip fracture, irreversible cognitive decompensation, and pneumonia.[57]
One of the most widely used drugs for controlling the behavior of people with dementia in Australia is the antipsychotic drug risperidone.[58] According to the Department of Health’s Therapeutic Goods Administration’s website, risperidone is allowed in older people with moderate to severe Alzheimer’s dementia for psychotic symptoms, or persistent agitation or aggression unresponsive to non-pharmacological approaches for up to 12 weeks.[59]
In an October 2019 letter to Human Rights Watch, the Department of Health also specified that “Australian guidelines acknowledge that non-pharmacological therapies are the first line treatment for behavioural and psychological disturbances in patients with dementia. However, if pharmacological therapy is required to control hallucinations, delusions or seriously disturbed behaviour, risperidone is considered first line therapy” (emphasis added).[60]
The product information for risperidone, posted on the Australian government’s Therapeutic Goods Administration’s website, notes that its use in older people with dementia increases their risk of death and stroke.[61] Other drugs of the same class of atypical antipsychotic drugs have this same language, but include an additional statement such as: “[This atypical antipsychotic] is not approved for the treatment of patients with dementia-related psychosis.”[62] Risperidone does not carry this statement in Australia. It does carry a black box warning in the United States, meaning that manufacturers must
include on conventional and atypical antipsychotic drug labels, including risperidone, that older patients with “dementia-related psychosis” treated with antipsychotic drugs are at an increased risk of death.[63]
Product Information on the Australian Government’s Department of
Therapeutic Goods Administration Website
|
Drug Name |
Class |
Product Information, including information on studies finding increased risk of death for use in older people with dementia |
Approved for Use in Older People with Dementia |
|
Olanzapine |
Atypical antipsychotic |
Yes[64] |
No[65] |
|
Risperidone and similar drugs |
Atypical antipsychotic |
Yes[66] |
Yes, for short-term (<12 week) use for people with Alzheimer’s[67] |
|
Quetiapine and similar drugs |
Atypical antipsychotic |
Yes[68] |
No[69] |
II. Use of Chemical Restraint in Aged Care Facilities
Through interviews with family members of people living or having lived in aged care facilities in Australia, Human Rights Watch documented the use of antipsychotic drugs and sedatives as chemical restraint on older people with dementia. The medicines were administered over long periods apparently to control and subdue people rather than ensure their well-being. Medicines were prescribed often at the request of nurses to doctors who were not physically present to evaluate the patients. Medicines were also often prescribed and administered without the informed consent of the individual or family members holding medical powers of attorney to make medical decisions on behalf of their loved ones. The practice of chemical restraint appears linked to both understaffing and a lack of staff trained in non-pharmacological, supportive interventions for people with dementia, as well as the absence of clear legal restrictions on this practice in Australian law.
The medicines being given to older people with dementia have been recognized by the Australian government’s Therapeutic Goods Authority as having serious risks of increased disability and death for older patients with dementia (see chart in Section I ). The potential for harm and lack of medical benefit for older people living in aged care facilities combined with the apparent intent of giving these medicines to control behaviors – without attempts to implement non-pharmacological interventions, indicates that this practice is chemical restraint.
We documented how aged care facility staff administered antipsychotic drugs, sedatives, opioids, and other drugs to residents. People were most commonly given the antipsychotic risperidone, often in combination with other drugs including, oxazepam, a sedative, and quetiapine, another antipsychotic.
Australian prescribing guidelines allow the use of risperidone in older people with Alzheimer’s after other interventions have been exhausted and only for 12 weeks.[70] We documented how aged care facility staff gave residents risperidone for periods beyond 12 weeks, in some cases for years. We also documented how staff gave older people antipsychotic medications that are approved for schizophrenia but are not approved for use in older people with dementia, such as olanzapine, also for weeks or months. None of the people who received these antipsychotic medications had a diagnosis of schizophrenia.
In all cases documented by Human Rights Watch in which relatives discussed the effects of the drugs with facility staff, interviewees told us how doctors or facility staff specified that the medication was given to control residents’ behavior. Staff reported to families that they did this in response to behavior such as wandering or trying to leave. Some people we interviewed said that staff chemically restrained their relatives for reportedly doing things such as moving around in their bed at night or having verbal outbursts.
This report documents the use of chemical restraints in situations where personal support was not provided to individuals to help manage their behavior over time. Staff gave older people with dementia these medications over periods of weeks, months, and years. Those interviewed did not include individuals with complaints about single uses of these drugs during crises or emergencies.
Interviewees described how formerly energetic, talkative people became lethargic and, in some cases, unable to speak, during the period that the drugs were administered. Many reported that their relatives slept heavily, often for long periods, and could not be awakened without difficulty. They experienced serious weight loss and dehydration, often because they were not able to stay awake long enough to eat or drink. Many became so weak from not using their muscles that they lost mobility. They often lost the ability to perform self-care tasks such as using the bathroom or showering.
According to family members, in no cases that we documented had staff secured the informed consent of individuals’ chosen person holding powers of attorney. In some cases, families learned that their relatives had been given antipsychotic or other medications only when they received the pharmacy bill. The CRPD Committee, the body of independent experts that monitors states’ compliance with the UN Convention on the Rights of Persons with Disabilities, has held that any treatment of an adult with medications without consent is a violation of the right to equal recognition before the law and an infringement of the right to personal integrity; freedom from torture and inhuman and degrading treatment; and freedom from violent exploitation and abuse.[71]
Some family members also told Human Rights Watch that they were able to have their older relatives go off the medicines that were restraining them by removing them from the facility, by caring for them at home with out-of-pocket support, or by hiring private staff in a facility, and that, with support, they were again able to enjoy things like being with loved ones, going for an outing, and listening to music.
Excessive Lethargy and Sleep
Lethargy and excessive sleep are some of the most significant effects of chemical restraints and which impact all other aspects of an individual’s life. “Glynnis,” 84, moved into an aged care facility on the Gold Coast in Queensland in 2017. She had dementia. About a year into her stay, Glynnis left the facility one morning and walked nine kilometers to her daughter’s house. After that, the facility told her family that it would give her medication to control her wandering but did not specify which drug or explain potential risks. Her granddaughter Katie told us that her family found out that the facility staff were giving Glynnis the antipsychotics after she took a photo of a chart left by a nurse in her grandmother’s room. Katie explained her grandmother’s condition after the medications started:
Everything about her, her health, her spirit, declined after that drug. We went to see her after the meds, and she couldn’t hold a conversation, she was dropping off to sleep, [just] like that. She wouldn’t get up to go to the toilet until the last second because she was so tired. She was having trouble getting out of the chairs, when she had no trouble before … She wasn’t moving at all. She had to be showered [by staff] … She was falling asleep sitting up. Having trouble getting up. Her eyes would roll back in her head.[72]
Together with an advocate from ADA Australia, an older person’s rights organization, Glynnis’s family met with the facility management and asked that they stop the medication. The facility refused. Katie said, “The more I pushed for no medications [as restraints], the more they resisted.”[73]
“Linda,” 59, has dementia and lives in an aged care facility in Melbourne, Victoria. Her daughter, “Jessica,” who has her mother’s power of attorney together with her siblings, told Human Rights Watch that in late 2018, Linda started walking restlessly around the facility and, in response, the staff gave her antipsychotic drugs that she had been prescribed PRN, pro re nata, meaning on an “as-needed” basis, determined by the staff, in addition to regular doses of medications. Jessica said staff had not informed her about the additional medications. She started to ask questions when she noticed her mother was going to sleep by 10 p.m., not waking until 11 a.m., and then falling asleep again at noon:
Two weeks ago, I found out she was getting oxazepam [a sedative] PRN almost every night. A nurse told me she was starting to get concerned [my mother] is [already] getting [a] 9 p.m. [dose of another sedative] every night.
So, I stayed and watched until 11 p.m. She was waking at 10:30 p.m. and moving around the bed, setting off the sensor.
I talked with the nurse, and his exact words were, “But I have to give her medication to keep her in bed.” I asked, “Could you give her a walk for 10 minutes?” He says, “At night, there are only two staff members on, I can’t give her a walk.”[74]
In 2018, staff at an aged care facility in Queensland reported to “Lisa” that her father, “Gene,” 85, had hit a nurse and would need to be placed “on tablets” to control him.[75] A general practitioner (GP) in the facility put him on three daily doses of antipsychotic drugs. Lisa found her father sleeping at all hours of the day. Staff reported to her that he fell asleep in the shower. She found a new GP who took him off the drugs, but Gene experienced lasting physical damage, as described below.[76]
Raylene Liddicoat, director of Simply Chronic Care, a nursing consultancy working in aged care facilities, told Human Rights Watch about an older woman in the facility where she worked who was “on medication to keep her in bed… She’d started to fall out of bed because she didn’t want to be alone in her room. So they wanted to sedate her. I said to the staff that we’ll get her up for her meals… This lady wants to be interactive with the community, not in bed.”[77]
Significant Weight Loss and Dehydration
Human Rights Watch documented several cases in which older people with dementia lost significant weight in aged care facilities while receiving medication used to restrain them.
For example, Michal Brown, a nurse, cared at home for her father, Lafras, who had Alzheimer’s disease. She has his power of attorney for his medical affairs. On April 11, 2017, she placed him in an aged care facility’s short-term respite program so that she could take a business trip. Brown came back from her trip three weeks later to find her father dramatically changed. “When I arrived, he was totally unresponsive – eyes closed, mouth open, pants half down, lying in a pool of urine,” she said. He had also lost significant weight. She complained in writing to the facility:
The shocking and marked difference in my father’s appearance of the man I brought in on 11 April to the man I saw on 1 May… His weight was 67 kilograms on entering the unit. I have finally been able to weigh him tonight, 3 [May] and he is weighing in at 58 kilograms! ... This weight was taken after having dad home for three days, of feeding my dad regular healthy meals. I would have like to have known his true weight on his return home on 1 May but due to his condition I have been unable to weigh him.[78]

A medication chart she later obtained appeared to be consistent with Lafras being given 0.5mg of the antipsychotic risperidone daily, double the amount she had given permission for, and half of a 15mg tablet of the sedative oxazepam initially, but later two full 15mg tablets per day. In her notes for the facility, it indicated that he could receive one oxazepam tablet if he became anxious but made clear that he should not be given it frequently, as he would sleep excessively for most of the next day.[79]
“Dean,” 75, has dementia and lives in an aged care facility in Northern Queensland. His wife, “Mae,” brings him breakfast and dinner each day, prompting him to eat each bite. She told Human Rights Watch that he cannot eat independently due to the medications he is on used to chemically restrain him for “behavior,” and staff do not take time to ensure he gets enough to eat.
Mae, who has her husband’s power of attorney, said her husband lost over 20 kilograms in his first five months at the aged care facility in 2017:
He was just sleeping when I was visiting before work and after work. I said he shouldn’t be on meds. I didn’t see him for two weeks because of a scabies outbreak [in the facility]. He lost two kilos. It’s a kilo a week if I don’t turn up with my meals.[80]
“Katie” told Human Rights Watch about her grandmother “Glynnis’s” serious weight loss and dehydration over about 18 months in 2017 and 2018 while she was on medication to restrain her in an aged care facility on the Gold Coast:
The weight loss started when she went on the drugs. She became gaunt. I was buying clothes for her, and she was always around a size 18. Then I had to buy size 12. I had to buy smaller bras for her. From an 18D down to a 14B. Every afternoon after work, I was going to feed her, and she was so dehydrated. They weren’t feeding her.
In October 2018 … they told us to say our goodbyes. So, I got my nurse friend to visit, and she gave [my grandmother] heaps of water, and then she could sit up. The nurse friend said she was dehydrated… She was skin and bone… Her collarbone was so far out. She hadn’t eaten or drunk for days.[81]
Glynnis recovered from the apparent dehydration but passed away two months later.
A geriatrician and neuropsychiatrist with more than 30 years’ experience working with people with dementia and other disabilities in Australia told Human Rights Watch of the negative impacts of chemical restraints:
I see [antipsychotic drugs] having a great impact on [older people’s] quality of life and physical health. And there usually isn’t a diagnosis to support these, so they are used as a chemical restraint, really.
The consequences are that we see otherwise healthy people develop horrible metabolic problems, diabetes, heart problems, stroke as a result of being on these psychotic medications. It’s all too common in the population I see of people with neurological disabilities [like dementia].
It’s a reflection of the fact that they have complex disabilities and the practitioners lack the expertise. It’s a question of making the right diagnosis and offering the right treatment, not just treatment to keep people’s behavior in line.[82]
Physical EffectsLouis, 68, has dementia, and his wife, Denise Fenech, holds his power of attorney. Fenech described how staff at the facility where he lives gave him drugs they said were to control his behavior: They said he grabbed staff and held someone against a wall… He threw a soup spoon… They called a psychiatrist in… In March 2018, I was told, not consulted, that they had started him [on new drugs]. They introduced drugs for agitation, and anxiety… When on the drugs, he immediately went into a neck spasm. [His head was] forced down onto his chest, causing headaches. It was hard to eat and drink. The physio[therapist] was concerned about a drug interaction…They said they stopped giving the drug to him, and it took several months of physio[therapy], a very gradual return.[83] |
Facilities’ Easy Access to Chemical Restraints
Registered nurses working in aged care homes, doctors, and pharmaceutical experts told Human Rights Watch that under current regulations in Australia, aged care facility staff may easily obtain the medications used in chemical restraint of older people. Facility staff can obtain a prescription for the medications used in chemical restraint, including antipsychotics, sedatives, and opioids, with a phone call at any time, day or night. Doctors can prescribe them without making an examination or even seeing the individual receiving the medications.
Raylene Liddicoat told Human Rights Watch about an illustrative experience while consulting at a facility, explaining how a staff member started her shift: “She hadn’t received handover, walked in, demanded the keys to the [medicines] cupboard, because she could see a lady escalated [agitated]. [She said,] “I’m not starting my shift because I know what she’s going to be like if I don’t give her her [diazepam] now.”[84]
Nurses or nursing assistants at facilities can ask that the prescription be issued with a PRN dosage. A PRN prescription means that the very people who are responsible for providing support to older people are the ones who can decide to give the person drugs instead of providing that support. As noted above, Human Rights Watch documented how older people in aged care facilities routinely received PRN medications.
Pamela, who has Alzheimer’s, was 72 in 2016 when staff at the aged care facility where she lived gave her risperidone PRN without the knowledge or informed consent of her daughter, who held her mother’s powers of attorney. Her daughter described an incident in which staff gave Pamela double the doctor’s prescribed maximum dose, which caused symptoms consistent with akathisia, “a state of agitation, distress, and restlessness that is an occasional side-effect of antipsychotic and antidepressant drugs.”[85] Pamela’s daughter described:
Mum is given risperidone, unconsented [without informed consent]. We knew nothing about it. To me, that was the attitude of the place. The following week I noticed a change, she was a little more lethargic. The following Friday I arrived to find her distressed in hallway, still in nightwear, her 1 p.m. lunch untouched.
By 9 p.m. that night, [the facility called me] to say that she’s so highly agitated, we are worried about staff safety, and have called an ambulance. She has feces all over her. She doesn’t want to lie in a bed. They go to strap her down. I said, “Don’t you dare.” They say, “Your mum’s on risperidone; we’ve given her two doses.”
They’ve [given her] four doses [of risperidone] in less than 24 hours. We didn’t know she was on it.[86]
Dr. Harry McConnell, a neuropsychiatrist and geriatrician with over 30 years of experience in aged care in Australia described seeing his patients with akathisia linked to antipsychotic drugs:
It’s an inner restlessness, to which an older person is particularly susceptible. When someone prescribes, they think they’re helping, but they cause the problem. Nothing will settle you down when you have [akathisia]. When you have language problems and cognitive problems it will make it very hard to express what’s going on. It manifests as anxiety and aggression.[87]
Raylene Liddicoat, director of Simply Chronic Care, a nursing consultancy working in aged care facilities, has been a nurse for 30 years, and in management and senior leadership roles in aged care facilities since 2008. She criticized the ease with which aged care facility staff can obtain PRN prescriptions for medications to manage residents’ behavior. She explained the process based on her long experience: “If a nurse writes the note saying the person was upset, that GP’s going to say, ‘Yes, I’ll put them on a PRN.’ I don’t like PRN medications as psychotropics. It’s probably helping the helper more than the resident.”[88]
Veronica, a practicing registered nurse (RN) in New South Wales who has worked in aged care for 20 years, told Human Rights Watch that often due to the lack of staffing and training, facility staff resort to medication when residents experience challenging behavior and that medications are easy to obtain. She said, “Nurses will ask for increases in medication because the only thing she has in her back pocket is pain meds… In aged care, you can reach a doctor over the phone for medications, with someone interpreting the patient for the doctor. The doctor may never see the person.”[89]
Veronica also noted that this does not have to be the practice. “In this facility, we don’t have anyone on PRNs,” she said. “There is more abuse with that. Medication is just not the answer. We need symptom management. [Facilities] don’t always have enough staff to support everyone.”[90]
Dr. McConnell, the geriatrician and neuropsychiatrist, explained the significant risks with PRNs:
There’s a huge problem with the PRN’s. I don’t really like using them… I don’t like using benzodiazepines [sedatives] and antipsychotic drugs as PRNs. [Often], you’ll see [a patient with] a regular dose, and then additional PRN’s of a similar medication. In a 24-hour period people can get quite a lot of medication that wasn’t intended. The effects of that are that person being over-sedated.[91]
Juanita Breen, a pharmacist and professor, told Human Rights Watch that her research on chemical restraints in aged care shows significant PRN use: “There is a lot of PRN use. It’s totally inappropriate, because usually the nurse decides when it’s being given, and may not refer to when it was [last] given, resulting in overdosing [too much medicine].”[92]
Facilities’ Responses to Complaints
Family members of people in aged care facilities described the difficulties they faced when raising concerns and complaints about chemical restraints with facility doctors, managers, and other staff. They talked about aged care administrators intimidating and attempting to force facility residents out. Other tactics included facility administrators applying to state guardianship bodies to remove persons with powers of attorney chosen by residents.
For example, Gene, 85, had dementia, and lived in a facility for one and a half years without being restrained. In January 2018, the facility told his daughter, Lisa, that he hit a nurse, and “needed tablets.” Lisa, who held powers of attorney for her father, said that the doctor and facility staff refused to acknowledge and address her concerns with his excessive sleeping, as detailed above, and instead pressured her to remove her father from the facility. At the meeting she requested with the doctor, she was shocked to find six other people at the meeting, beside the doctor: the lifestyle manager, duty manager, registered nurse, manager, assistant manager, and clinical nurse manager. She said:
I was alone in the meeting. They were intimidating. They were saying that if I didn’t allow for this [he could move out]. The doctor said: “Oh, there’s another [aged care facility] that would take him that is more culturally appropriate.” (My father speaks Italian.) They suggested a far [away] home. I said it was too far. The doctor said “Well, you don’t have to walk there.”[93]
In another case, “Chloe” talked about reprisals from the staff when she filed a formal complaint about medication use for her mother, “Judy,” 91, whom Chloe had found unresponsive in her dementia unit’s lounge in November 2018. Chloe told Human Rights Watch:
I made an incident report, with their form. I used the form from the intake packet. After that, I told the GP working [at the aged care facility I didn’t want her restrained on drugs]. The doctor said she couldn’t [stop] it, but she could halve it. She said she needed a wean.
After this, the nurses gave me a hard time. Two nurses approached me to say [my mother] was aggressive and needed more medications… [But I saw that] she hasn’t had an aggressive episode since halving the drugs. She still walks quite well and sweeps her floor there… She was worse on the medications, but they wouldn’t admit it.[94]
Chloe also called the Mental Health Commission in Queensland in January 2019, regarding chemical restraint of her mother. The commission referred her to ADA Australia for advocacy support with the facility and a few months later visited the facility and investigated. At a meeting with the facility staff shortly after the investigation, a nurse told Chloe to “get the commissioner off our backs.” At the time of the interview with Human Rights Watch, Chloe had not been given any information about the outcome of the investigation.[95] Judy is still living in this facility.
Mark Viney told Human Rights Watch about the response of the facility in Queensland where his father lived after Viney made two formal complaints to the Aged Care Complaints Commission in 2017 about chemical restraint of his father:
The general manager at the next meeting… started making out I was making it impossible for them to do their jobs. The regional manager said I’m being unreasonable, asking for carers to do more things…
I put in a complaint to the federal government body… The facility swore in an affidavit that they weren’t trying to get rid of dad.
In January 2018, ADA [Aged and Disability Advocacy Australia] came to help… ADA Australia told me that the facility had contacted the Adult Guardian of Queensland to try to have me removed as my father’s guardian. I actually never saw anything; ADA Australia told me. [Fortunately] their submission didn’t go anywhere.[96]
Staff in aged care facilities described different approaches to staff complaints. One facility manager told Human Rights Watch that if a resident or family member has a concern, then the manager will ask that they meet, together with other relevant staff. This manager indicated that she also recommends a family mediation service, rather than the government-designated aged care advocacy service.[97] A nurse working at another facility said that they give each new resident and their family members information about complaints systems and advocacy services and that it is also included in the patient handbook that each resident receives.[98]
Informed Consent
In the cases documented by Human Rights Watch, doctors, nurses, and other facility staff did not ask for consent for medications that were used to chemically restrain people or from any individuals receiving the medications. Also, medical personnel often did not seek informed consent from relatives, who in all the cases that we documented had a power of attorney to make health decisions. Several interviewees described to Human Rights Watch the shock and confusion they experienced when they learned about medications given to their relatives only when they received chemist (pharmacy) bills for the medications or otherwise happened upon medical records. Some interviewees said that facility staff gave medications even when family members holding powers of attorney specifically refused.
Laws on informed consent are complex in Australia and governed by state and territory legislation.[99] Health departments for most states and territories issue guidelines on some form of consent for health care.[100] However, there is no clarity on requirements for obtaining informed consent for medical treatment in aged care facilities.
In the October 2019 letter to Human Rights Watch, the Department of Health said, “The responsibility for seeking informed consent of the consumer or their family for prescription of medications, including psychotropics, rests with the prescriber (rather than the approved provider).”[101] The department further specified that an aged care provider “has no power to impose the obligation to seek informed consent on visiting medical practitioners or nurse practitioners.”[102]
At the same time, the Aged Care (Single Quality Framework) Reform Act, 2018, a regulation that applies to all aged care facilities that receive Commonwealth government funding,[103] requires that, “Each consumer is supported to exercise choice and independence, including to: (i) make decisions about their own care.”[104] An example it offers in guidance to providers of aged care services, is “Consumers say the organisation supports them to make decisions affecting their health and well-being.”[105]
Australia’s international legal obligations require informed consent for all medical treatment and interventions, as a fundamental aspect of human dignity, bodily integrity, and freedom from torture and ill-treatment.[106] For persons who may wish to have support in making decisions, the government should ensure that this is available. Forms of support are detailed below in International Standards.
“Marie” said she knew something was deeply wrong after returning from holiday to find her mother unconscious and strapped by her stomach to a chair in the aged care facility in Southern Queensland. She had her mother’s power of attorney, and decided to investigate her care more closely:
I looked on the chemists’ bills… I see [new drugs] started when we went away. I rang the chemist, who said, “[The drug] is to calm people down.” As I’m going through [more bills]; I see it again…
I rang the doctor, saying, “You prescribed risperidone. Could you explain why?” Because the nurses tell him to. On the strength of what the nursing staff told him.
I got information from the internet, printed the [United States government] black box warning that said it would [increase risk of] death. They said, “That’s American.” I went directly to each nursing staff with the black box warning. They kept restraining after I said not to.[107]
Mae said that she discovered that staff were chemically restraining her husband, Dean, who lives in an aged care facility in Northern Queensland, whose case is described in more detail above. She had learned he was on olanzepine PRN (a sedative), endone (a narcotic pain reliever), and tramadol (a narcotic-like pain reliever) after checking the pharmacy bill and discussing it with her general practitioner in March 2018.
She then started meeting with facility staff and doctor, together with an advocate, asking that they stop using the drugs. In September 2018, she took her husband home for a visit and saw that the facility sent him home with endone and targin (a narcotic pain reliever). After Mae’s repeated meetings with the facility staff, in February 2019, they agreed to begin reducing some of the drugs by lowering the dosage. Mae said that once they decreased the dosage, Dean was “actually having a life” and able to walk with support. At the time of the interview with Human Rights Watch, the facility had not fully stopped all chemical restraints.[108]
Ray Ekins’ daughter, Susan, who holds her father’s powers of attorney, found that he was on antipsychotic medication. She had asked the geriatrician about his drastic emotional and physical changes, as described above, and the doctor made no mention of medication. She investigated further:
I asked for his medical chart to be sent to a new doctor I was working for as a receptionist. It came across my desk. Olanzepine is contraindicated for people with dementia, and it causes Parkinsonian symptoms. He had been on it for 15 months! We moved him immediately, and got him a new GP, and weaned him off them.[109]
In some cases, nursing staff and doctors gave patients medication even after relatives with powers of attorney forbade it. For example, David Viney, 88, has mild dementia and has had a major stroke. He gave his son, Mark, an enduring power of attorney for his medical affairs. In 2017, the facility’s geriatrician placed David Viney on quetiapine, an antipsychotic, which caused him to sleep excessively and have difficulty eating.
Mark complained to his father’s GP, who acceded to Mark’s request that his father no longer receive quetiapine or any medications to control him. Three months later, the facility’s geriatrician prescribed new, sedating medications, without the informed consent of David or Mark Viney. The geriatrician called Mark after prescribing them, angry that he and the general practitioner had not followed his earlier prescription:
He said, “Who do you think you are? Where’s your medical degree from? Good luck getting him off the drug I put him on.” I told him not to see my dad again.
At 2 p.m. the next day, they [aged care facility staff] came to give my dad meds. The staff told me that the doctor upped his dose to four times per day. She said, “I have to give it to him.” I said, “No you don’t. I have the PoA [power of attorney], and I asked my father, and he refused it.”[110]
As noted below, a new manager began working at the facility and David Viney is no longer being chemically restrained.
In some cases, staff at aged care facilities hid from relatives the fact that they were giving certain medications to an older person. Katie told Human Rights Watch that she learned in December 2017 that her grandmother was being given drugs that caused sedation after her grandmother had wandered out of the facility:
I spoke with [clinical nurse manager], who said … we were told by this lady [the manager at the facility] that the drugs would be the best thing, that we would be harming her [without them]. We were not told anything about antipsychotic drugs…
[She told me:] “It’s harmless medication. Ninety percent of our patients here are on these. It will be beneficial. Reduce stress levels. It may be a very small amount of[diazepam].”
[Later,] her chart was left by a nurse. I opened it and took a photo and showed my doctor. She was actually on quite a high dose of an antipsychotic, plus [diazepam]. The doctor was incensed because they had taken her off all of her other medications for her cholesterol, and heart medication. My doctor said the dose [of the antipsychotic] was quite high.[111]
Life after Chemical Restraints
Some family members told Human Rights Watch that they were able to have their relatives weaned off medications used to restrain them, by moving them to a different facility or back home, working with a different doctor, or, in one case, hiring an aide. They described how their relatives no longer slept excessively and could communicate and engage in daily activities more.
One husband said he and his family fought for his wife, Monica, whom he lives with in a facility near Melbourne, to be weaned off the drugs used to restrain her. They share a room in the facility, and he holds her power of attorney. He saw how staff gave her the medications when she cried out, wandered around the facility and did not sit still, disrupting the staff in their routines. After extensive negotiation, Monica’s doctor and facility staff agreed to wean her from the medicines after he paid for a private carer to stay with her in the facility 13 hours each day. He said his wife went from being hunched and unbalanced, to being able to sit, eat, greet people, and dance when her grandson visits and sings.[112]
Their son told Human Rights Watch,
On medication, her essence was gone. She could not lay down, had restless legs… I couldn’t calm her down. She’d be hollering and wailing… When she was on heavy medications, she wasn’t [engaging in group activities like] playing with balloons. When she was off, she could play with them. Interacting brought her to life.[113]
David Viney, 88, has mild dementia and has had a major stroke. Staff at a facility put him on chemical restraints after which he slept all day and had difficulty eating, swallowing, and sitting upright. When his son, Mark, complained, the facility took him off the drugs, and according to him, his father recovered significantly:
They stopped the drugs, and he was himself again by the end of three days. He was telling jokes and laughing. I hadn’t seen him that way for months. He can remember things. They didn’t want to take him off the drugs. I said I don’t want him on. Told them to cease.[114]
Ray Ekins, 78, has dementia and was discharged from a hospital after surgery in 2013 back to the aged care facility where he had been living. At the hospital, doctors had prescribed a new prescription for olanzepine, an antipsychotic prohibited for use in older people with dementia, to be given three times per day. His daughter, Susan, recalled the changes after the medication started:
At that stage he couldn’t walk, only shuffle, he was very, very depressed, just crying all the time. And he couldn’t swallow… He would say, “My mind is a hell to me.” He wouldn’t be engaged in a conversation… All his symptoms are side effects of the antipsychotics, and they disappeared after he went off.[115]
Susan asked his geriatrician about these significant changes, who told her that her father was old, and she and Ray would just have to accept it. Unable to change the doctor’s decision, Susan moved him to a new facility in 2014, which weaned him off the medications immediately. She described the change:
Now, he’s very, very much like his old self. He’s Irish, with a thick Irish accent, and he’s hilarious. He’s very funny. He likes to just go out and have lunch. We’ll often take a picnic. We’ll go for walks on the beach. If there’s music on in a pub, we’ll go in the afternoon, when he’s not too tired.[116]

“Elsa,” whose mother lost significant weight while on quetiapine, an antipsychotic, moved her mother to a new facility 2014, and the staff there agreed to take her off the drugs. Elsa described the improvements in her mother, but also lasting consequences:
She never really recovered from the drugs. She never got mobile again… She’d lost all her muscle tone, any muscles that could hold her up vertically were gone… She did perk up; we could take her out in the sunshine, and she would enjoy it. She was a lot more alert, but she lost her mobility in amongst it all.[117]
When Gene’s daughter saw that he was sleeping during morning and afternoon visits while on medications to control his behavior, as described above, she found a different doctor who took him off the drugs. Her father never fully recovered, however:
My dad was off all drugs, but he wasn’t even swallowing. The doctor took him off [the drugs] and said, “I think [the medications] made him unable to swallow.” My dad didn’t regain that ability.
The new doctor said he had had a big stroke and lots of little strokes [while on the medications]. He said this three weeks before my dad died [of stroke].[118]
III. Experiences with Government Complaint Mechanisms
People can make complaints about treatment, conditions, or other issues in aged care facilities to the Aged Care Quality and Safety Commission (ACQSC) (formerly known as the Aged Care Complaints Commissioner), the primary government agency responsible for monitoring aged care in Australia.[119] It receives complaints and accredits according to the Aged Care Quality Standards for Australian government-funded aged care services by accrediting, assessing, monitoring, and resolving complaints received regarding subsidized aged care services.[120] Starting in January 2020, it will also incorporate “aged care approval and compliance functions” from the Department of Health.[121]
The ACQSC can take the following actions in response to complaints: 1) early resolution, whereby the ACQSC advises the complainant, calls the service provider, or takes other similar steps; 2) refer the complaint to a service provider to address; 3) facilitate a resolution with the service provider and complainant; or 4) conduct an investigation.[122] The ACQSC may also ask the complainant and service provider to undergo a formal mediation process external to the ACQSC with an independent mediator.[123] Engaging with an independent mediator involves a separate cost, one that the complainant and the service provider “would need to discuss and agree to.”[124] In its October 2019 letter to Human Rights Watch, the Department of Health stated that the ACQSC notifies it of any findings of non-compliance and the department may take regulatory action, including imposing sanctions. However, the department did not provide further detail as to the nature or frequency of such sanctions.[125]
Individuals can also file complaints in the case of death with the local coroner, the Australian Department of Health or, local entities such as a health ombudsman, department of health, or in some places the local human rights commission, depending on the state or territory, or the police.[126] Coroners investigate the cause of death in individual cases warranting an inquiry, and in some instances, conduct inquests into multiple deaths where similar factors may have contributed to each death. Their reports and recommendations can serve to highlight systemic issues.[127] A person who has a complaint about a doctor or nurse, including about inappropriate prescribing, may complain to the Australian Health Practitioner Regulation Agency (AHPRA). Sanctions may be imposed against a doctor or nurse if their conduct is found to fall short of statutory standards.[128]
The ACQSC closed 5,738 complaints in the year ending June 30, 2018. Seventy-five percent of the complaints were about residential aged care. The remainder came from other areas it oversees, such as home care.[129] Complaints are finalized with a final decision. This may be with an agreement or other document stating that the concerns have been resolved between the complainant and the facility or the ACQSC believes the issues to have been addressed. If the ACQSC believes the service provider is not meeting its responsibilities, it may direct the service provider to make changes. The concern can be referred to the ACQSC Quality Assessment and Monitoring Group for other action, such as a compliance inspection or audit. It can also be referred to the Department of Health for further examination of compliance with the law and regulations.[130]
In its October 2019 letter to Human Rights Watch, the Department of Health stated that the ACQSC “assesses the use of chemical restraint during complaint handling processes,” as well as during its accreditation, assessment, and monitoring (see additional details below regarding the ACQSC). It said there were a total of 44 complaints about chemical restraint in 2018 and 18 in the first quarter of 2019. The department did not provide any information regarding the specific actions taken or outcomes of these complaints.[131]
A complainant unsatisfied with a decision can request that the ACQSC review it again; or send a complaint to the ACQSC about how it managed the complaint; or ask the Commonwealth Ombudsman to review the ACQSC actions in the complaint process.[132]
Family members of aged care facility residents who filed complaints about chemical restraint to the Aged Care Complaints Commissioner (ACCC, as of January 2019, the ACQSC) and other agencies described that in some cases, complaint mechanisms were difficult to use. Some other family members said complaints officers referred them back to the facility, with complaints not being resolved.
For example, “Estelle,” 90, has dementia, and has been living in an aged care facility in Queensland since September 2016. In January 2018, she fell while on risperidone. Her daughter “Imogen,” who has her power of attorney, put in a complaint about the use of medication and the accident to the ACCC (now the ACQSC). Imogen told us:
I lost faith in [the ACCC] because they are supposed to be there for the resident, but I don’t think they fought enough. They didn’t investigate, just rang up the facility. I would use ACCC as a resource, but I wouldn’t rely on it. They believed the facility over me.
I went to my federal MP [member of parliament] – I wanted an appointment. They said to complain to the ACCC. When we complained, we were shut down.[133]
“Marie’s” 99-year-old mother had been given risperidone without her knowledge or informed consent in a facility on the Gold Coast. She had additional complaints about the facility using a physical restraint and inadequate numbers of staff to support residents to eat at mealtimes. She explained her experience when she called to file a complaint in 2016:
I rang up the Queensland Aged Care Ombudsman [now the Aged Care Quality and Safety Commission]. They were so rude I was in tears. They said, “You’ve got three [complaints], and you can only have one,” and she was angry. She said, “Make up your mind! You can have just the [complaint about] risperidone, the restraint on your mother’s stomach, or not feeding her.” It was cruel. I just left it.[134]
Katie told Human Rights Watch about her difficulty finding out how to file a complaint and initiating a complaint regarding treatment of her grandmother, including sleeping excessively all day while on medications, serious weight loss, and other concerns in November 2017. “It took two days to get it started,” she said. “It’s not easy. I rung them, emails, wait for calls back.”[135]
The complaints officer of Queensland Aged Care Complaints Commissioner
responded to Katie in an email that she would contact the aged care facility and ask a manager to meet with her and “ask the provider to report back to me with the agreed outcomes.”[136] Katie met with the facility manager, and the manager told her they would change her grandmother’s medications, but not stop them as Katie requested. She said, “They said they were going to cut out some medications and leave others. The chemist said [Glynnis] was on a lot more medications, and I spoke to with the doctor, who confirmed.”
Katie said that after this exchange, “The aged care complaints outcome? They simply said what the manager said… Aged care contacted me two months later. I told them I wasn’t happy with the outcome, and that they didn’t follow through. They told me I could put in a new complaint. After that, I just did everything myself.”[137] She started going to the facility daily to feed her grandmother, who was too sleepy to eat while on the medications.
Mark Viney said that he made two complaints to the Aged Care Complaints Commission (ACCC) (now the ACQSC) in mid-2017 and early 2018 about heavy sedation of his father, and the facility’s efforts to remove his father from the facility. “[I] put in another complaint [in 2018] to government saying, ‘They’re still trying to get rid of him,’” Viney said. “Complaints said they would help, then they went on holiday.”[138] They never contacted Viney again. He said that a new manager started at the facility and staff are no longer sedating his father.
“Jessica” went to great lengths to try to stop chemical restraint of her mother “Linda,” who has dementia and has lived in a facility since 2015. Jessica first raised the medications issue, among others, directly with the facility staff in 2017, who refused to make changes. She then filed complaints with the ACCC in May 2017. The commission responded by instructing her to meet with the facility staff again. She described that September 2017 meeting:
[My family] had a meeting with the facility… We went in with heaps of evidence, so we went in wanting a response from the provider with solutions. They sat down and talked in circles. The CEO … said, “We are not here to talk about the future. We are here to talk about what is in your complaint.”[139]
The facility staff refused to stop using the chemical restraints. After she filed a second complaint in March 2018, the commission visited the site. The commission closed the second complaint in January 2019 without requiring the facility to make any changes. She said, “it’s frustrating, they didn’t do much.”[140]
Jessica then tried to speak with an accrediting officer from the Aged Care Quality and Safety Commission during the government agency’s re-accreditation for the facility, hoping this might spur a resolution:
I knew accreditation was coming; I was hoping our issues would be picked up. They were only accredited to April 2019. When I met with the accreditor, instead of sitting down and hearing my concerns, [he told me how I should] deal with the facility manager. I brought all this evidence, meetings, emails, showing how we used internal feedback forms, trying to resolve it internally … I have complaint fatigue. And a fear of reprisals [from the facility].[141]
The facility had threatened to bring a bullying case against her, after she raised her voice with a nurse, having stayed up all night caring for her mother. “[The facility CEO] tried to frame it as a workplace health and safety issue,” she said. “As if you come in here and speak inappropriately to staff it threatens their safety.” She has asked for this to be formalized in order to be given the right of reply. At the time of the interview with Human Rights Watch, the facility had not acted against Jessica.[142]
In June 2017, Julie McAdams made a formal complaint to the Aged Care Complaints Commission about the “heavy sedation” of her mother, Avis Gross, 90, by staff at the aged care facility where she lived. The commission did not examine her case but referred her to the Australian Health Practitioner Regulation Agency (AHPRA) saying that psychotropic medications prescribed by a doctor was not within its jurisdiction. She complained again in November 2018, shortly before her mother passed away, and they again did not intervene.[143]
In December 2018, McAdams complained to the Commonwealth Ombudsman about what she saw as unsatisfactory responses she received from the Complaints Commission. In January 2019, the ombudsman’s office declined to investigate, finding nothing wrong with the commission’s actions. McAdams then appealed for a procedural review of the Commonwealth Ombudsman’s decision. The internal review concluded there were no problems with the way its office had handled her complaint.[144]
“Amber” filed a complaint with the Australian Health Practitioner Regulation Agency (AHPRA) about the doctor who prescribed drugs used to chemically restrain her mother “Phillipa,” 95, in an aged care facility. She had called the in-house doctor for the facility to ask about the drugs, and she said that he said that “he only prescribed what the nursing home told him.”[145]
The existing model of complaints does not appear to be uniformly addressing the complaints of older people in aged care facilities to a unified, high standard, and complaint mechanisms are no substitute for strong regulation that is fully enforced to protect older people from chemical restraint.
IV. Government Response
The Australian government has acknowledged problems in the aged care sector and taken some steps to reform. These steps include a Royal Commission of Inquiry into Aged Care Quality and Safety, a new regulation on physical and chemical restraint, and revised principles and guidance for providers of aged care services. Australia’s Council of Attorneys General has also created a National Plan to Respond to the Abuse of Older Australians, which includes chemical restraint in its commonly recognized forms of abuse.[146] However, these steps have not resulted in prohibitions on the use of chemical restraint, allowing staff of aged care institutions to continue this practice.
In September 2018, Prime Minister Scott Morrison announced a Royal Commission of Inquiry into Aged Care Quality and Safety (the Royal Commission).[147] It is tasked with examining the quality of aged care services and how these services currently meet the needs of older people; mistreatment and “all forms of abuse,” and how to best deliver services to “the increasing number of Australians living with dementia.”[148] The Royal Commission has been conducting hearings in towns and cities across the country and has received thousands of submissions from individuals and organizations.[149] Chemical restraint is one area of inquiry.[150] The Royal Commission is expected to deliver its final report in April 2020.
Aged Care Quality and Safety Commission
In 2019, the Aged Care Quality and Safety Commission (ACQSC) revised its guidelines for aged care providers, known as the Aged Care Quality Standards. The User Rights Amendment (Charter of Aged Care Rights) Principles 2019, also amends the Quality of Care Principles, 2014. The government has issued guidance on this in the form of the Aged Care Quality Standards. The revised standards acknowledge the problems of chemical restraint but allow their use. Regarding antipsychotic medicines, the guidelines state:
There is concern that these medicines are being prescribed inappropriately in people aged 65 years and over for their sedative effects – that is, as a form of chemical restraint for people with psychological and behavioural symptoms of dementia or delirium.[151] ... If an organisation uses restrictive practices such as physical or chemical restraint, these are expected to be consistent with best practice and used as a last resort, for as short a time as possible and comply with relevant legislation.[152]
Each aged care provider is to determine its own best practices.[153]
The 2019 Aged Care Quality Standards do not require facilities to report their use of chemical restraint. They only require that facilities demonstrate “a clinical guidance framework including ... minimising the use of restraint.”[154] The standards require providers to self-report three quality indicators: pressure injuries; the use of physical restraint; and unplanned weight loss.[155]
The ACQSC is responsible for inspections of facilities and monitors implementation of the Aged Care Quality Standards.[156] Quality assessors began unannounced visits to aged care facilities for the first time in 2019.[157] Of the 249 ACQSC site audits of aged care facilities in the first quarter of 2019, behavioral management was the second most frequent “not met” outcome, and clinical care was the fourth most frequent “not met” outcome.[158] The Department of Health reported to Human Rights Watch that in 2018, medication management was one of the five most frequent “not met” outcomes in residential care audits, and the most complained about issue. The department did not provide any details about chemical restraint findings from the ACQSC audits.[159]
Currently, it has the power to revoke accreditation of a service, meaning that they are unable to receive Commonwealth subsidies. From January 1, 2020 it will have compliance and enforcement functions, which currently remain with the Department of Health.[160]
Failure to Prohibit Chemical Restraint
Australian commonwealth laws do not prohibit chemical restraint. In July 2019, a new regulation issued by the Commonwealth Minister for Senior Australians and Aged Care, drafted by the Department of Health, purports to minimize the use of physical and chemical restraint. It set restrictions on physical restraints, including an explicit requirement for consent to their use, unless necessary in an emergency. It did not set those same limits and obligations regarding chemical restraints.[161] It amends the Quality of Care Principles 2014, the animating regulation for the Aged Care Act. Instead of eliminating the use of chemical restraint, the regulation tries to regulate the practice.
The regulation allows aged care facility staff to use chemical restraint for anyone in aged care if a health practitioner has assessed an individual as “requiring the restraint” and has prescribed the relevant medication. It requires the decision to use the restraint to be documented but does not require prior informed consent of the person or a representative, such as a family member. It says the representative should be notified in advance “if it is practicable to do so.” According to the October 2019 letter from the Department of Health to Human Rights Watch, referring to aged care facilities responsibilities under the regulation, providers must “inform the consumer’s representative around the time of administering the medication.”[162] The regulation does not state that this representative must be the individual’s chosen proxy, such as a person they have given powers of attorney.
The Department of Health stated at a parliamentary hearing about Minimising the Use of Restraints Principles 2019, that it does not regulate prescribing practices, and therefore does not regulate informed consent, safeguards, or a requirement of alternatives.[163] Other regulatory agencies, namely the National Disability Insurance Scheme, have chosen to regulate the practice of chemical restraint, including these prescribing practices, informed consent, safeguards and the requirement of alternative measures, among others.[164]
Pharmacists, lawyers, and policy experts have criticized the regulations for failing to prohibit chemical restraint, perpetuating the use of restraints to control people’s behavior, and failing to include a requirement for informed consent and provisions to allow for refusal.[165] The rules also do not include any specifications about complaints and recourse – there is no penalty or sanctions specified for facilities or staff that inappropriately administer medication. The regulation does not specify which entity is tasked with monitoring it.
The government does not have a clear policy plan to eliminate chemical restraint. In the October 2019 letter from the Department of Health to Human Rights Watch, the department noted that the Australian government spent AU$4.1 million (US$2.7 million) between 2013 and 2016 on projects to reduce “the use of sedative and antipsychotic medications in residential aged care facilities.”[166] In 2019, however, the letter states, the department’s focus is on education and “messaging,” including on the “appropriate use” of these drugs in aged care facilities as well as messaging on “alternative management strategies for behavioural and psychological symptoms of dementia….”[167]
In a July 2019 letter to Human Rights Watch, Leading Age Services Australia, a trade association of aged care providers, said chemical restraint should be a last resort, but appeared to acknowledge that not all providers implement this in practice:
In LASA’s view, the principle that restraint should be a last resort is widely accepted across the sector. There are few age services providers that would not support the principle of minimising the use of restraint. However, there is variation in the way that providers are able to operationalise the principle of minimising restraint.[168]
Failure to Set Effective Standards for Supportive Levels of Staffing
The Australian government has yet to ensure standards for supportive levels of staffing and training of staff in aged care facilities. Families of older people with dementia told us how low numbers of staff negatively affected the quality of care and increased the use of chemical restraints. Aged care facility staff, including registered nurses, reported the difficulties of providing adequate care due to limited staff.
Australian law does not require a minimum number of staff hours per person per day or a minimum number of staff in aged care facilities. Aged care providers must ensure staffing be “adequate” and “appropriately skilled.”[169]
The right to health requires governments to ensure that health services are appropriate and of good quality.[170] The Australian Nursing and Midwifery Federation, the Australian Medical Association, the Royal Australian College of General Practitioners, and the Australia and New Zealand Society for Geriatric Medicine wrote in a letter urging legislation on staffing in aged care that “Studies identify that the main reason for missed care, or low-quality care in residential aged care facilities is that there is not enough staff available.”[171] Numerous studies around the world have shown that adequate staffing—sufficient quantity, training, and consistency of staff—is critically important to the quality of care aged care facility residents receive, and that inadequate staffing leads to substandard care.[172] Gross understaffing and under-training of staff may contribute to the use of chemical restraint.
Elsa, a former nurse, said that her mother, 86, who has dementia, was chemically restrained in an aged care facility in New South Wales in 2014. Elsa described how she would visit her mother to find her lying in soiled diapers, with the nurse call bell unanswered:
In the high care facility, there were maybe 100 [residents]. I would only ever see a maximum of four staff. [T]here were times I went to visit my mom and she was sitting in urine and feces, had been for a long time, and the light was on. It was on numerous occasions. When she rang the buzzer to go to the toilet, no one would come.[173]
A registered nurse with more than 40 years of experience told Human Rights Watch about how he felt compelled to leave his job in an aged care facility due to low staffing and the pressure and risk he experienced:
I resigned late last year, reluctantly, because my license was at risk... It’s impossible to supervise the numbers [of residents]. I worked every Sunday, with close to 80 or 90 residents, and no other RN [registered nurse] staff on Sunday… RNs were responsible for medication management; that consumed most of my day…
I was worried about what I’d find when I got there at 6 a.m. One shift starts at six, another ends. The providers don’t allow handover. There are falls, medications, messages from families, visits from doctors. But you’ve got to hit the ground running, and you can’t [take time to] go through [handover] notes.
I’d looked after one gentleman I’ve known for many years. He was dying. I simply didn’t have the time to spend with him that day I was working. It was very saddening. He was a lovely mate, and finally I just couldn’t provide the care I felt I needed with him. The only real time I had to spend with him was after my shift. It was going to hell in a handbasket.[174]
A registered nurse working in several aged care facilities across New South Wales described the low staffing that she typically encountered in her daily work:
In a hospital, the ratio of RN to patient is one nurse for three or four patients. In aged care it’s two care staff to 30 residents, and one RN for 200 residents, in different facilities. How are you supposed to effectively provide service? All it takes is two people to fall out of bed, or one person to be transitioning back to the facility from the hospital, and all the care staff is tied up. Staff is always stretched in the current environment.[175]
The Australian Nursing and Midwifery Federation’s National Aged Care Survey 2019 found that nearly 90 percent of aged care staff reported current staffing levels at their facility were not able to provide an adequate standard of nursing and personal care to residents. Problems with dementia management were one of the top concerns of aged care facility staff.[176]
Training of aged care staff is another key area of concern. One carer working in an aged care facility in Northern Queensland told Human Rights Watch about the training she receives: “There’s in-house training for hygiene and lifting, but not dementia. Every six months there’s a refresher. Nothing about dementia.”[177] A physical therapist with almost nine years of experience in aged care noted, “There is mandatory training for all staff on fire safety, infection prevention, and physical handling. There is no formal mandated training on behavior management. It’s up to the provider.”[178]
Juanita Breen, a pharmacist who has studied chemical restraint in aged care facilities in Australia, noted that staff levels and appropriate training are essential to move away from the use of chemical restraints. She said, “If we eliminate restraints, we need a workforce that understands how to manage dementia. There is no training for the workforce. I think it’s such a complex problem: legislation is needed and underlying that there needs to be a lot of education.”[179]
One study of a training for bathing people with dementia in the United States found it produced a statistically significant reduction in agitated behavior and antipsychotic drug use.[180]
Aged and Community Services Australia, a trade association for non-profit aged care providers, said in a letter to Human Rights Watch regarding the issue of staffing requirements:
- We do not support fixed staffing ratios in residential facilities for a variety of reasons, including:
- Facilities and variable acuity levels, both within facilities over time and between different facilities;
- Fixed ratios do not account for the variety of differing service models within the sector; and
- Fixed ratios do not account for other factors such as building design, technology etc.
- However we support appropriate staffing levels underpinned by an appropriate skills mix and timely access to a responsive external health professional and specialist workforce.[181]
Older Australians should have the right to be free from chemical restraint. They should have easy access to complaint mechanisms empowered to address complaints about chemical restraint. Older people with dementia should have support from trained staff at properly staffed aged care facilities to file a complaint if they request such assistance.
The existing of government response to chemical restraint has been lacking. A regulation currently permits chemical restraints; the complaints system, though changed, still lacks navigability and has been unclear in its authority to address complaints of chemical restraint; broader systemic issues of undertraining and understaffing at aged care facilities persist.
V. International Standards and Australian Law
International Standards
Prohibition of Torture and Other Cruel, Inhuman, and Degrading Treatment
Australia is party to several international conventions that prohibit torture and other cruel, inhuman or degrading treatment or punishment, including the International Covenant on Civil and Political Rights, the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, and the Convention on the Rights of People with Disabilities (CRPD).[182]
People living in aged care facilities, particularly those with dementia or other similar illnesses or conditions, are persons with disabilities for the purposes of the CRPD, in that they are people who “have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others.”[183]
In its 2013 review of Australia, the United Nations Committee on the Rights of Persons with Disabilities, which monitors state compliance with the CRPD, criticized the use of chemical restraints in relation to Australia’s obligations to prohibit torture and ill treatment. It noted that, “persons with disabilities, particularly those with intellectual impairment or psychosocial disability, are subjected to unregulated behaviour modification or restrictive practices such as chemical, mechanical and physical restraints and seclusion, in various environments.”[184] The committee recommended that Australia take immediate steps to end restrictive practices, including by establishing an independent national preventive mechanism to monitor places where they may occur, to ensure that persons with disabilities are “not subjected to intrusive medical interventions.”[185]
In 2013, Juan Mendez, then the UN special rapporteur on torture and other cruel, inhuman or degrading treatment or punishment, warned of the danger of human rights violations in the healthcare setting where the perception persists that “certain practices in health-care may be defended by the authorities on grounds of administrative efficiency, behaviour modification or medical necessity.”[186] Mendez also noted that “medical treatments of an intrusive and irreversible nature, when lacking a therapeutic purpose, may constitute torture or ill-treatment when enforced or administered without the free and informed consent of the person concerned.”[187] He also emphasized that an act may constitute ill-treatment, even if it is “intended to benefit the ‘patient’” and may “exist alongside ostensibly therapeutic aims.”[188]
Mendez stated that such violations of rights are particularly likely to occur when the “treatments are performed on patients from marginalized groups, such as persons with disabilities, notwithstanding claims of good intentions or medical necessity.”[189] He also stated that the use of a “prolonged restraint” may constitute torture and ill-treatment when used against people with mental (psychosocial or intellectual) disabilities.[190]
Mendez concluded that “it is essential that an absolute ban on all coercive and non-consensual measures, including restraint and solitary confinement of people with psychosocial or intellectual disabilities, should apply in all places of deprivation of liberty, including in psychiatric and social care institutions.”[191]
Right to Health and Informed Consent
The right to the highest attainable standard of physical and mental health is enshrined in several international human rights conventions to which Australia is party, including the International Covenant on Economic, Social and Cultural Rights and the CRPD.[192]
In accordance with the right to health, governments have a core obligation to ensure the right of access to health care on a non-discriminatory basis, especially for vulnerable or marginalized groups.[193] Governments also may violate the right to health through the failure to take appropriate steps towards the full realization of everyone’s right to health.[194] Allowing aged care facilities to give antipsychotic medications for purposes other than the benefit of the recipient, especially over an extended period of time, is inconsistent with the right to health. It poses threats to life and well-being from adverse side effects and increased mortality associated with antipsychotic use.
The CRPD requires informed consent for medical treatment and interventions. [195] The CRPD committee has determined that treating an adult with medications without consent is a violation of the right to equal recognition before the law, [196] the right to personal integrity, and the right to freedom from violent exploitation and abuse, as well as the right to freedom from torture and inhuman and degrading treatment.[197]
For persons who may require support in making decisions and giving their informed consent for medical treatment, support should be provided and can take different forms. These can include:
- Accessibility measures and reasonable accommodation in understanding medical interventions, their consequences and side effects, as well as alternatives;
- Advance directives; and
- The appointment of one or more support persons chosen by the person concerned.
The CRPD Committee has acknowledged that in some cases, even after serious and sustainable efforts have been made, it may not be possible to determine a person’s will and preferences, due to communication barriers or for other reasons. This may be the case with some people with dementia. In such situations, every effort should be made to make the “best interpretation” of an individual’s will and preferences.[198] Consideration should be given to all forms of verbal or nonverbal communication, as well as a person’s relevant previously manifested preferences, values, attitudes, and actions.
The special rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health has expressed that informed consent “is a core element of the right to health, both as a freedom and an integral safeguard to its enjoyment.”[199] In a 2009 report the special rapporteur noted:
Informed consent is not mere acceptance of a medical intervention, but a voluntary and sufficiently informed decision, protecting the right of the patient to be involved in medical decision-making, and assigning associated duties and obligations to health-care providers… [It promotes] patient autonomy, self-determination, bodily integrity and well-being.[200]
The special rapporteur on torture has similarly noted that informed consent is fundamental to “respecting an individual’s autonomy, self-determination and human dignity.”[201]
The special rapporteur on the right to health called on states to:
[R]adically reduce medical coercion… [and] not to permit [others] to provide consent on behalf of persons with disabilities on decisions that concern their physical or mental integrity; instead, support should be provided at all times for them to make decisions, including in emergency and crisis situations.[202]
The special rapporteur acknowledged that such change was “a challenging process that will take time” but that “deliberate, targeted, and concrete actions” were needed to end medical interventions without informed consent:
(a) Mainstream alternatives to coercion in policy with a view to legal reform;
(b) Develop a well-stocked basket of non-coercive alternatives in practice;
(c) Develop a road map to radically reduce coercive medical practices, with a view to their elimination, with the participation of diverse stakeholders, including rights holders;
(d) Establish an exchange of good practices between and within countries;
(e) Scale up research investment and quantitative and qualitative data collection to monitor progress towards these goals.[203]
Key Domestic Laws
The Australian Parliamentary Joint Committee on Human Rights
The Australian Parliamentary Joint Committee on Human Rights, which examines bills, legislation and regulations for compatibility with international human rights standards, said in December 2018 with regard to specific legislation in the disability support services sector that the use of restrictive practices, including chemical restraint, “may amount to torture, cruel, inhuman or degrading treatment or punishment,” recognizing that “Australia’s obligations in relation to torture, cruel, inhuman or degrading treatment or punishment are absolute (that is, they can never be subject to limitations).”[204] The Parliamentary Joint Committee on Human Rights has also said that the use of restrictive practices (including chemical restraint) can infringe on the right to liberty and security of the person, guaranteed by the International Covenant on Civil and Political Rights and the CRPD, as well as the following rights guaranteed under the CRPD: the right to equal recognition before the law and to exercise legal capacity; the right to respect for their physical and mental integrity on an equal basis with others; the right to freedom from exploitation, violence and abuse; and the right to freedom of expression and access to information.[205]
Of the three Australian states where Human Rights Watch conducted research, only one currently regulates chemical restraint in some form. In New South Wales, the Guardianship Act and advanced care directives apply to the provision of medical treatment in hospital settings and aged care facilities. Consent for the provision of medical treatment is generally required, though medical treatment may be carried out on an individual without consent in certain circumstances.[206] It defines special medical treatment for the purpose of the Guardianship Act and includes any treatment that involves the use of an aversive stimulus, whether mechanical, chemical, physical or otherwise. Only the New South Wales Civil and Administrative Tribunal can consent to special treatment.[207] Victoria’s legal framework does not regulate the use of chemical restraints in aged care facilities. Queensland does not regulate chemical restraint in aged care facilities.[208]
In Australian criminal and tort law, giving a sedating medication without consent or other legal or medical justification (such as pursuant to a court order or for emergency treatment), may be a crime, a civil wrong (a tort), or both.[209] Human Rights Watch is not aware of any Australian prosecution or civil suit in relation to chemical restraint.
Prohibitions on Age Discrimination
Australian national laws prohibit discrimination based on age or based on disability in certain circumstances. Each of the Australian states and territories also have laws prohibiting age discrimination and disability discrimination in certain circumstances.[210] The Age Discrimination Act 2004 prohibits age discrimination in certain circumstances, including in the provision of services and accommodation.[211] Under the act, direct age discrimination occurs when a person is treated less favorably than a person of a different age would be treated in the same circumstances, because of their age or a characteristic that pertains to, or is generally imputed to, persons of their age.[212] Indirect age discrimination occurs if an unreasonable condition, requirement or practice is imposed to the disadvantage of persons of a specific age.[213]
Giving drugs that chemically restrain older persons will constitute unlawful age discrimination under Australian law if an aged care facility would not give the medication to a younger person in the same circumstances, or unreasonably maintains the practice of giving medications to older persons.
Prohibitions on Disability Discrimination
The Disability Discrimination Act 1992 prohibits discrimination on the basis of disability, which under law includes dementia, in the provision of services or accommodation.[214] Under the act, direct discrimination occurs if a person with a disability is treated less favorably than a person without the disability would be treated in circumstances that are not materially different, including where there is a failure to make reasonable adjustments for the person with a disability.[215] Indirect discrimination occurs where an unreasonable requirement or condition is imposed that a person with a disability is not able to comply with, to the person’s disadvantage, including where reasonable adjustments are not made to facilitate compliance.[216]
Chemically restraining a person with dementia or a similar disability will constitute unlawful disability discrimination under Australian law if an aged care facility would not give antipsychotic medication to a person who behaved in a similar manner but did not have dementia or a similar disability. Such discrimination might occur if, for example, a person with dementia is subject to a chemical restraint as a result of behavior deemed aggressive, where a person without dementia, behaving similarly, would not be subject to a chemical restraint. Further, the use of chemical restraints may constitute unlawful discrimination if reasonable adjustments, such as moving a person away from another resident whose behavior is causing the person agitation, or calming them through other techniques, are not used in preference to chemical restraint.
VI. Recommendations
To the Minister for Aged Care and Senior Australians
- Introduce legislation to prohibit the use of chemical restraints as means of controlling the behavior of older people with dementia or for the convenience of staff.
- Any new law should also ensure:
- Informed consent for all treatment or interventions;
- Independent monitoring; and
- Effective, accessible, independent complaint mechanisms.
- Ensure all policies and actions implemented for aged care are consistent with the UN Convention on the Rights of Persons with Disabilities.
- Develop more community-based services for older people with dementia to ensure support for older people to live independently in their communities, including at home.
To Parliament
- Pass legislation to prohibit the use of drugs as chemical restraints as means of controlling the behavior of older people with dementia or for the convenience of staff. The legislation should include:
- Prohibition of the use of chemical restraints and outline penalties;
- Requirement of informed consent for all treatments and interventions from the older person or, where that is not possible, a relative chosen by them;
- Mandatory training for all aged care facility staff in dementia and alternative methods and skills to de-escalate unwanted behavior and support the needs of people with dementia;
- Adequate minimum staffing levels to provide support to older people;
- Adequate enforcement mechanisms to protect older people’s rights;
- Independent monitoring and oversight of all facilities without obstacles;
- Effective, accessible, independent complaint mechanisms, including for individuals in aged care and their families;
- An amendment to the Aged Care Act to expressly grant access to aged care facilities to advocates and quality assessors.
- Consider an Aged Care Ombudsman role, tasked with assisting Australians using the Aged Care system, and making policy recommendations, completely independent from the Department of Health and the Aged Care Quality and Safety Commission.
To the Department of Health
- Strengthen the regulatory environment to end use of chemical restraint by addressing the following areas:
Ensure Free and Informed Consent:
- Require a standardized protocol for obtaining free and informed consent from the individual whose care is concerned, including with support as needed in the decision, or the appointed representative of a person with dementia, as long as this representative is chosen freely and tasked with reflecting the individual’s will and preferences before, during, and for the continuation of medical treatment.
- Ensure meaningful penalties for failure to obtain informed consent.
- Develop and implement models of supported decision-making to enable people using aged care services to make their own decisions about treatment and care.
- Implement programs that ensure equitable access to preventative, diagnostic and care services for all people with dementia, including social and rehabilitative support.
- Introduce national and local public health and awareness campaigns to reduce stigma around dementia.
- Ensure strong protections against eviction of older people from aged care facilities to better protect them from coercive threats of eviction.
For Adequate Minimum Staffing in Aged Care Facilities:
- Require a 24/7 registered nurse presence in all aged care facilities and establish stronger minimum staffing levels and ratios or other enforceable minimum requirements to ensure continuous, person-centered support for older people in aged care.
- Consider automatic penalties for facilities that do not meet minimum quantitative and qualitative staffing requirements.
- Ensure adequate staffing to support older people.
- Require training for all aged care facility staff in dementia support. Trainings should include how to recognize and analyze behaviors, verbal de-escalation techniques, tools to interact effectively with people with dementia, and side effects of medication.
For Ending Chemical Restraint:
- Consider creating a new inspection survey protocol that can identify and document problems potentially arising from chemical restraint, for example, excessive sleeping, and problems around a lack of free and informed consent in accepting medications, and monitoring, proactively interviewing staff, residents, and residents’ families.
- Ensure strong protections for whistleblowers to report chemical restraint.
- Eliminate the permitted use of risperidone as a chemical restraint.
- Eliminate the use of PRN for drugs known to be used as chemical restraints.
To the Aged Care Quality and Safety Commission
- Ensure complaints officers are empowered to investigate and address complaints of chemical restraint.
- Ensure that inspections and monitoring assessors proactively and confidentially interview older people, residents’ families, and staff to identify indications of chemical restraint.
- Publish data regarding chemical restraint findings, including numbers of allegations, investigations, and closed cases, facility names, and the amounts of fines or other penalties for this practice.
To the Council of Attorneys General
- Establish legal support services for older people experiencing chemical restraint as a part of the National Plan to Respond to the Abuse of Older Australians, in coordination with existing state advocacy organizations.
To State and Territory Governments
- Prohibit the use of chemical restraints as means of controlling the behavior of older people with dementia or for the convenience of staff. Ensure minimum staffing and adequate training in aged care facilities to support older people.
To the Coroner in Each State and Territory:
- Review deaths that occur in nursing homes to assess whether use of chemical restraints may have contributed to the death. Where appropriate, conduct inquiries or inquests into such deaths.
Acknowledgements
This report was researched and written by Bethany Brown, researcher on older people’s rights in Human Rights Watch’s Disability Rights Division. Giorgi Gogia, associate director in the Europe and Central Asia Division; Jane Buchanan, deputy director in the Disability Rights Division; Elaine Pearson, Australia director at Human Rights Watch; Nicole Tooby, Australia coordinator at Human Rights Watch, and Laura Thomas, a former fellow at Human Rights Watch, provided research support.
The report was edited by Jane Buchanan, Elaine Pearson, and Joe Amon, a consultant on public health. Babatunde Olugboji, deputy program director, and James Ross, legal and policy director, provided programmatic and legal review respectively.
Cara Schulte, associate in the Disability Rights Division, provided research and production assistance. Layout and production were done by Cara Schulte; Jose Martinez, senior coordinator; Fitzroy Hepkins, production manager; and Remington Arthur, publications associate. Fortune Nyasha Nyamande, Mariam Matta, and Stephanie Mao, fellows and interns on older people’s rights, and Jinseul Jun, intern with the Disability Rights Division, provided additional research support. Lawyers acting on a pro bono basis helped us review pertinent domestic legislation.
This work would not have been possible without generosity and courage of so many individuals with family in facilities, people living in facilities, and their advocates, as well as facility staff. We are grateful to the many advocates, medical professionals, and scholars who shared their knowledge and experience with us.
This report would not be what it is without the support of ADA Australia’s team: Geoff Rowe, Karen Williams, and Jess Ma. Kaele Stokes and Sally Lambourne and their team at Dementia Australia supported this work throughout Victoria and New South Wales.
Human Rights Watch would also like to thank the many human rights organizations, activists, lawyers, and health professionals working in the field of older people’s rights and aged care who shared their insights and analyses with us or otherwise provided assistance.
Bill Mitchell of Townsville Legal Centre provided valuable legal background.
We would also like to thank ACT Disability and Aged Care Advocacy (ADACAS); Julie Reeves, the Australian Nursing and Midwifery Federation; Scott McDougall, formerly with Caxton Legal Centre and Cybele Koning, Caxton Legal Centre; Carmelle Peisah, Capacity Australia; Donna Swan, COTA Victoria; Kate Swaffer, Dementia Alliance International; Michael Gourlay, Pauline Meaney and Kate Dalton, Elder Rights Advocacy; Lise Barry, Macquarie University; Joe Ibrahim, Monash University; Amanda Alford, National Association of Community Legal Centres; Craig Gear, Older Persons Advocacy Network; Mary Burgess, Queensland Office of the Public Advocate; Natalie Siegel-Brown, Queensland Office of the Public Guardian; Margaret Duckett, Russell Westacott and Pat Joyce, Seniors Rights Service; Raylene Liddicoat, Simply Chronic Care; Andrew Byrnes, University of New South Wales; Terry Carney, University of Sydney; Juanita Breen, University of Tasmania; Nola Ries, Linda Steele, University of Technology Sydney; Lyn Phillipson, University of Wollongong; Lauren Adamson, John Chesterman, Victoria Office of the Public Advocate, and many others including those not identified by name to protect confidentiality.
Collier Charitable Fund generously supported this work. A special thank you to the Planet Wheeler Foundation for the financial support that made this research and report possible. Human Rights Watch would like to thank the Samuel Centre for Social Connectedness for its partnership throughout this research. Social connectedness is a guiding theme in Human Rights Watch’s work for older people’s human rights. We offer our deepest thanks to Kim Samuel for her unwavering belief in the power of social connectedness.
Annex
Glossary
Aged care facility is a residential facility in which a person resides, where they receive personal care or nursing care, or both, with appropriate staffing to meet residents’ nursing and personal care needs. These facilities also provide meals and cleaning services, furnishings, furniture, and equipment for residents.
Aged Care Quality and Safety Commission (ACQSC) began operations on January 1, 2019, as the primary government agency responsible for monitoring aged care in Australia. It replaced the Australian Aged Care Quality Agency and the Aged Care Complaints Commissioner. It accredits, monitors, assesses, and receives complaints regarding government-subsidized aged care services.
Australian Health Practitioners Regulation Agency (APHRA) is a governmental body supporting the national boards of health professions. It accepts complaints about practitioners’ behavior placing the public at risk or practicing their profession in an unsafe way.
Australian Department of Health develops and delivers policies and programs and advises the Australian government on health, aged care, and sport. It seeks to ensure better health for all Australians.
Chemical restraint is restraint that is, or that involves, the use of medication or a chemical substance for the purpose of influencing a person’s behavior other than medication prescribed for the treatment of, or to enable treatment of, a diagnosed mental health condition or intellectual disability, a physical illness, or a physical condition.
Commonwealth Ombudsman assesses complaints about the actions of Australian government agencies and private sector organizations it oversees, to consider if the actions were wrong, unjust, unlawful, discriminatory, or unfair.
Dementia is the loss of cognitive functioning—thinking, remembering, and reasoning—and behavioral abilities to such an extent that it interferes with a person's daily life and activities.
Informed Consent is a decision made with a full understanding of the purpose, risks, benefits, and alternatives to a medical intervention, in the absence of pressure or coercion.
Person-centered care is care focused on an individual’s unique qualities as a person. Such care builds and nurtures relationships between the individual and others.
Pharmacists and chemists are used interchangeably in Australia to refer generally to professionals trained and authorized to dispense medicines. However, formally, a pharmacist is qualified to prepare and dispense medicines, and a chemist is a broader term for an expert in chemistry. Chemist can also refer to a drugstore.
Power of attorney is a legal document in which one person nominates and gives legal authority to another to act on affairs on their behalf.
Quality Assessors conduct assessments in aged care facilities and have the authority to enter and search facilities. They work for the ACQSC (above) and are distinct from ACQSC complaints officers.
Risperidone is an antipsychotic medicine that is used to treat schizophrenia in adults and children who are at least 13 years old. In Australia, it is permitted for the treatment (up to 12 weeks) of psychotic symptoms, or persistent agitation or aggression unresponsive to non-pharmacological approaches in patients with moderate to severe dementia of the Alzheimer type. Risperidone is not approved by the Food and Drug Administration (FDA) in the United States for the treatment of behavior problems in older adults with dementia.
Royal Commission of Inquiry into Aged Care Quality and Safety was created by the Australian government in September 2018. It is holding hearings across the country and accepts submissions from the public to learn about aged care. It will conclude its activities in April 2020 with a final report making recommendations for improving aged care services.
